|
This past spring I read a fascinating book, “Death Interrupted”, written by Dr. Blair Bigham. Within the book, Bigham shares his journey of trying to make sense of what he calls the “death dilemma” that happens for doctors, patients, and their families as they wrestle with the question of when is it the right time to allow death to happen. Bigham shares interesting stories of medical history but also many personal stories from his own medical experience as a paramedic and then an Intensive Care Unit (ICU) doctor as well as stories from his research for this book that makes his book very compelling and enjoyable to read. I resonated quite deeply with many of the issues he raised in this book for they are very present in my palliative care ministry. In this blog, I plan to provide a detail summary of his book, sharing his key insights into what has created this death dilemma along with his conclusion to resolving it.  The History of Medical Intervention In his early job as a paramedic, Bigham followed what was called Death Policy 4.4 which described the “obvious dead” as people who were pulseless, breathless, and lifeless and had a certain dead person look (11). When he encountered such dead people as a paramedic, he knew that there was nothing to do. Yet, sometimes it was not so clear for the death look had not appeared yet and so the race was on to pull the person back from the cliff of death through cardiopulmonary resuscitation (CPR) and other medical interventions like defibrillation (12). When he became an Emergency Room (ER) doctor, the obviously dead never came to the ER and so he never encountered a patient who met the clear criteria of Policy 4.4 (17). Now, the decision to declare death was his. And here is where he experienced head on the death dilemma. Now he “encounter almost daily situations where the life I’m entrusted with can’t be saved, but where death is anything but black and white” (23). The death dilemma is a recent phenomenon. Going back a hundred years, doctors were not typically present when a person died. Furthermore, Bigham notes, death was a common experience with global life expectancy being around 30 years in the 1800’s, while in 2000 this global life expectancy was 70 with some countries having life expectancies over 80 (35). Furthermore, death happened in people’s home so it was part of people’s everyday experience, not hidden away in hospitals or other health institutions. Between 1850 and 1950, Bigham concludes, life expectancy doubled due to vaccines, antibiotics, and public health measures like clean water and simple hygiene (36). I (Gord), personally, was surprised how doctors, by simply washing their hands before helping a mother give birth, led to a dramatic drop in babies and mother dying soon after childhood (36-37).  Since 1950, we have seen huge changes in medical technology that has raised the death dilemma into the forefront. In 1952, during a polio epidemic in Denmark, Bigham learned, they discovered that ventilators dropped the fatality rate of polio from 80% to 40% (45). Soon after, ventilators popped up around the world. At first these ventilators were hand-driven but soon they were mechanized and “devices were eventually sequestered together forming the first intensive care units” (45). (see picture above; polio patients in Boston ER room, 1955) Soon after, in 1960, Guy Knickerbocker published findings in 1960 about cardiopulmonary resuscitation (CPR) and CPR quickly became the medical standard for patients whose hearts had stopped (48). At the about same time, Bigham discovered, Knickerbocker developed the defibrillator. “As defibrillators became smaller [and thus portable] and CPR was taught to medical students around the world and as ventilators became common place, doctors became appreciating the life-saving implications of applying invasive therapies to people at the brink of death” (49). “By the end of the 1960’s, the word resuscitation was mainstream, and intensive care units had been established in most hospitals for diseases other than just polio” (49). Now, Bigham notes, we have medical technologies to do the work of many of our organs: lungs (ventilator), kidney (kidney dialysis), feeding tubes (stomach), urostomy (bladder) , colostomy (bowels), heart machine, etc. (61-62). Now, “I can take nearly every aspect of your physiology” and address the problem with medical technology. “Most times, I win this battle with death …but there are times I lose. A slow decompensation, one organ at a time, into oblivion...The problem is this: there comes a point where I know I will lose, but I don’t know exactly when. There won’t be a return to life, but the line of death hasn’t been crossed. It is no-man’s land, where no person ever wants to be” (62). Furthermore, Bigham highlights that “all this technology makes it quite hard to actually die, but none of it gives assurances that you will recover” (70). In fact, “the treatment for one failed organ often makes another worst” (70). What makes it even more complicated is that each machine is owned by a different specialist in the hospital but no one except the internist holds the full picture who often is forced to make trade-offs between the different specialists to ensure each organ has a fighting chance (71). This begs the question, how do we avoid this situation that places us right in the centre of the death dilemma? In some sense, Bigham concludes that “the death dilemma is a result of our often indiscriminate application of technology to prevent in the short-term a death that will ultimately come anyway” (68). What does it mean to die? To explore this grey zone further, Bigham turns to the question, “how do we know death has occurred?” Before this death dilemma appeared, death was primarily determined through checking if the heart had stopped beating and had no hope of being restarted. However, with the invention of ventilators, brain dead people no longer died quickly (71). To determine if a person was brain dead, the ventilator had to be shut off, but this raised another concern due to the emergence of organ transplants. Organs often became damaged waiting for death to happen so that these organs could be transplanted. This led, Bigham asserts, to “the urgency to precisely determine death while on ventilator: solid organ transplant was quickly becoming available, and fresh organs were in high demand” (72). The criteria for brain dead needed to be defined. 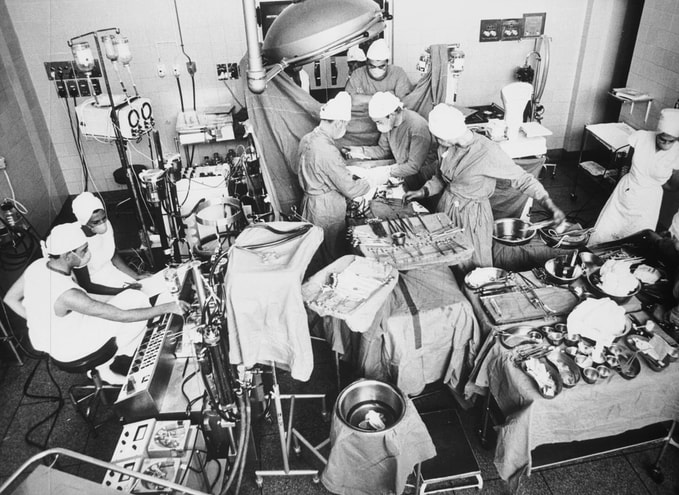 The first human heart transplant happened in South Africa in 1967, but there was no established brain dead criteria (74). The second heart transplant was done in Japan months later, but the transplant doctor was charged for manslaughter. These charges were later dropped but repeated criminal accusations plagued Japanese doctors (76). This legal controversy, Bigham notes, was occurring around the world. Most of the heart transplants were unsuccessful so few places were doing heart transplants until the arrival of anti-rejection medications made heart transplants viable again (77). The brain dead controversy eventually led to the Uniform Determination of Death Act (81) which stressed both the personhood and the physical brain of person. “When the brain dies, it is when the soul departed: what is left are ‘mortal remains’” (81). However, this Death Act didn’t resolve the controversy for many religious people saw the soul based in the heart, not the brain. This difference, Bigham claims, led to conflict between families who couldn’t make a decision and the transplant medical people who needed that organ right away (84). Bigham then researches why families have a hard time with the reality of death. One of his sources, Steve Berry, death historian, states that death is no longer a common experience of most people, but instead has “been exotified and denied to such an extreme that the idea of discontinuity of the self is so harrowing to people” (87) Furthermore, Berry claims that when people are treated as special and deserving of life, death seems unacceptable (85). He argues further that we are having an epistemic crisis, where due to our smartphones, we think we can access the facts ourselves, and so we have lost public confidence in all forms of authority, government, medicine, technology, etc. (86). Seeing these factors, no wonder people in our culture fight death to the end causing us to "spend ¼ of all health care dollars in the last six months of life” (89). Bigham discovered that there are “over one hundred thousand technology-dependent patients in long-term facilities in the United States, pushed out of hospitals no longer willing to deal with the consequences of their treatments” (92). “Chronic critical illness in the U.S. is a twenty-five billion industry” (93). Bigham believes that ”while aging population is no doubt a large part of it, therapeutic advances that decrease ICU death rates without getting people back to health are major contributing factors” (93). The costs caused by this death dilemma are very clear, and they are both emotional and economic (93).  Eventually, brain death became defined as the death of the brain stem and the irreversible loss of [the capacity of] consciousness” (98) or personhood (99). “When neurological death is proven to have occurred, personhood has ended” (100). In 2006, three guidelines were formulated to diagnose brain death, and to be verified by two physicians. One, ”you must have a reason to be brain dead” (100). Two “you must not have any confounding factors that could be mimicking brain death”(101). Lastly, ”a detailed exam of the cranial nerves must be performed” (101). While this provides a scientific definition of death, Bigham, through his research, discovered that there can be clash between families and medical staff. Families need time to transition from hope to despair, and that is something, Bigham observes, that doctors are not good at (108). Candi Cann, Professor of Religion and death researcher, sees “a void in the system that religious leaders can fill, offering guidance at end of life that can help normalize the dying process while doctors are trying to overcome it” (127). The Root of the Death Dilemma It is at this point in the book that Bigham begins to summarize what he thinks creates the death dilemma. He sees it being caused by technology, resuscitation glorification and death denialism. (145). Bigham describes "’resuscitation glorification’ as a societal belief that death is never near, if it comes at all, and that survival is always better than death, a position many in the know would dispute” (144). The end result of these factors is false hope, which Bigham sees at the centre of the death dilemma. This false hope, Bigham argues, "sets aside one of the most important tools in medicine, palliative care, until the window for effective palliative measures has mostly closed and it is too late to undo extraordinarily suffering” (145). From here, Bigham begins to unpack the culture found within the ICU. While families wrestle with the fear of death, doctor wrestle with the fear of failure (146). A fear of failure requires a humility within a doctor to admit that they cannot help a patient (148). Bigham highlights that “doctors are trained to look at things they can fix, establishing a self-esteem system based on making things better” (151). Therefore, for most doctors, the fear of failure is tied to their fear of death for death is seen as the “only bad outcome one can experience from surgery” (149) ..."when in delaying death, we may only cause more pain, more suffering, more despair” (149).  Because of these fears, Bigham notes that “for many specialties, the palliative care conversation is a non-starter”(157). “Many surgeons consider a move to involve palliative care experts as 'giving up’ and in many ways it is. But it isn’t giving up on the patient; it is giving up on a curative intent and on fighting a reality that can’t be avoided” (157). Bigham highlights that emergency doctors have a process called “flipping the plan” which describes “conversations they have with families of patients who aren’t suitable for full resuscitation efforts” (164). These doctors realize that there is some point where “you have to turn off the curative tap and turn on the palliative tap” (165). With cancer, this changepoint is more obvious: when chemotherapy treatments stop, you then move to palliative (166). However, this natural process of slow death that happens openly in palliative care is foreign to many people who expect sudden death. For example, “with heart failure, they get a pacemaker, and then they get an LVAD (left ventricular assist device), so they were dying the whole time, but it’s so medicalized that when these technologies fail, death than comes quickly. It’s not that you’re here one minute and then you’re gone“ (165). One of the interesting findings from Bigham’s research is that families based their decisions around death on the spiritual realm. While doctors flood them with more data and science when they are in this indecisive place, families are often looking for some sign that death is meant to happen (167). A Good Death Since there is such reluctance to talk about dying and death within the medical system, Bigham explores what a good death might look like. Interestingly, Bigham discovered that “only 25% of people have taken steps to ensure their wishes are known and 7 percent had spoken to their doctor” (180). When you lose capacity and are no longer able to share your wishes, it is the role of your Power of Attorney around Personal Care or close family members to share your wishes. These wishes around dying are called Advanced Directives, a conversation that I (Gord) am often privy to or encouraging in my palliative care ministry as a spiritual care provider.  It is pretty hard to have a good death when no knows what you consider a good death for you to be. Bigham has observed that “time and time again, families in the ICU are able to clearly articulate that 'Mom would never want this' yet can’t bring themselves to let go, to let those wishes be acted upon by the medical team” (187). In describing a good death means that a “bad death” is also a reality. One of Bigham’s research sources compared the ICU to a water treatment plant. Just as water issues upstream are eventually discovered downstream in a water treatment plant, everything that goes wrong in the health care system eventually gets to the ICU (193). As a result, the ICU source said, “I am a big believer that there is a negative quality of life” (193) which means in this context, a life that is no longer worth living and thus leads to a bad death. Bigham concludes that death happens in four ways when we are caught in this death dilemma. The ICU staff will work “full throttle until your heart gives out despite all the drugs, shocks, and chest compressions” (197). Second, “your brain can swell until blood can’t get it, and you’ll be pronounced brain dead” (197). Third, you can choose to assign people in your life, and arm them with documentation (Advance Care Directives), to make sure you never end up on unhelpful technology to begin with and move to palliative care (197). Or fourth, “you (or more likely someone acting on your behalf) can flip the plan at which point we’ll keep you comfortable (and probably comatose) while the machines are peeled off and you die naturally” (199). This option is often called palliative sedation. In recent years, Medical Assistance in Dying (MAiD) or euthanasia has entered the equation. For many, Bigham notes, “euthanasia is a way to avoid the pains doctors today can extoll on people as they near the end of their lives. Afraid to wither away, they instead choose a controlled—if not early—death away from the institutions and machines that define modern medicine (211). Often, Bigham learned from a MAiD practitioner, “good palliative care means people don’t want MAiD right away. But there comes a times when they are suffering too much, despite all that palliative care can offer” (204).  The Technology Conundrum Knowing the reality of a “bad death” and “good death” only sharpens the death dilemma. It is clear decision-making needs to happen but it is “not always clear who will live and who will die when we make decisions about implementing medical technology” (235), especially when “doctors around the globe are pushing the limits of resuscitation, often with remarkable results” (236). Bigham stresses that “as technology gets better, there is even more hope, more optimism, that resuscitation can save a life. But what happens when we roll the dice and lose?” (236). Bigham has observed that “every ICU has its frequent flyers, its bounce-backs and chronic long-haulers , the patient who has been there for one hundred, two hundred, three hundred days” (238). Eventually death comes to chronic ICU residents for they can only linger so long for eventually you will end up suffering from complications (243). Seeing this death dilemma so sharply, Bigham wonders “how could we differentiate false hope from true hope?” (255). Unfortunately, the reality is, “that ability to prognosticate about survival and future quality of life are inherently limited and will always create a tension that needs to be addressed incorporating uncertainty” (255). Toward the end of his book, Bigham has a big “aha” moment. “In the ICU, the doctors knew the dismal prognosis and so did the family, but neither was willing to make the difficult call to lessen, not maximize, the use of technology that would, in all likelihood, only temporary postpone death” (257). Bigham wondered, “could I, [as their doctor], simply make the interpretation on behalf of my patients, based on what their families could tell me, and propose ending the use of technology?” (257). Wouldn’t that solve the death dilemma? He learned from a senior physician that “some family members want us to take responsibility for these decisions and – in the right circumstances –we should be willing to do that” (256). In the end, Bigham realizes, that to resolve this death dilemma, we need to first “move technology from its current power grabbing position and instead consider its use when ethical -- and by ethical, I mean not only to prevent immediate death but to reasonably promote a return to life” (271-272).  Preventing immediate death is not, by itself, a valid enough reason to apply life-saving technology (272). Once this happens, Bigham claims we see that there are three major players in the death dilemma…and none involve medical technology: the patient, the patient’s family, and the medical staff. Each of these players have the ability to end the death dilemma (271): the patient through having a clear plan of care around their health and dying, the family through not placing unreasonable demands on doctors due to grief and unrealistic hopes, and medical staff through not losing sight of the forest of the reality of life and death due to the trees of symptoms demanding their attention (271).
Bigham, Blaire. Death Interrupted: How modern medicine is complicating the way we die. Toronto: House of Anansi Press, 2022. Gord Alton MDiv RP CASC Supervisor-Educator
0 Comments
|
 RSS Feed
RSS Feed
